15 Solid Reasons to Try EMDR (Eye Movement Desensitization and Reprocessing)
Eye Movement Desensitization and Reprocessing (EMDR) is a structured psychotherapy most often used for trauma, PTSD, and distress that still feels “stuck.”
It is designed to help the brain and body process painful experiences so they feel less overwhelming and less disruptive in the present.
EMDR is not magic, and it is not the right fit for every person in every moment, but many people consider it because they want a more direct, focused way of working through material that continues to affect daily life.
This guide is meant to help someone who is curious about EMDR, searching online for clear information, or trying to decide whether it may be worth discussing with a therapist.
How to use this guide
Use this guide if you are trying to understand what EMDR therapy is, why people try it, what a session is like, what the research says, and when EMDR may not be the best next step.
15 Solid Reasons to Try EMDR Therapy
These reasons to try EMDR are not guarantees, and they are not a diagnosis. They are common patterns that lead people to search for EMDR, ask questions about it, or bring it up with a therapist.
1. Trauma still feels active.
Some people try EMDR therapy because past experiences do not feel fully “past.” Even when they know the event is over, their body still reacts as if the danger is present.
EMDR is often considered when intrusive memories, emotional spikes, or physical stress reactions continue to show up long after something happened.
2. You avoid reminders, and it is shrinking your life.
Avoidance can quietly take over daily life. A person may stop going places, having conversations, or engaging in situations that feel loaded.
EMDR may be worth considering when avoidance has become a coping strategy that is understandable but costly.
3. You understand the problem, but still feel stuck.
Insight is helpful, but insight alone does not always create change. Many people understand why they react the way they do, yet the reaction remains the same
EMDR may be useful when a person feels intellectually aware but emotionally unchanged.
4. Your body reacts before your words can catch up.
For some people, the problem does not show up first as a thought. It shows up as panic, shutdown, tightness, numbness, nausea, or a fast nervous-system alarm.
EMDR can be appealing when the issue feels stored in the body as much as in the mind.
5. Shame keeps returning.
A person may keep circling painful beliefs such as “I am not enough,” “I am weak,” or “It was my fault.”
EMDR is often considered when a painful memory has become linked to a negative self-belief that keeps resurfacing despite reassurance or reflection.
6. Old experiences keep affecting current relationships.
Past wounds can shape present trust, closeness, anger, fear, or conflict.
People sometimes pursue EMDR when they notice that their reactions in current relationships feel bigger, faster, or more rigid than the present situation alone would explain.
7. You are tired of reliving the past.
Nightmares, emotional replays, flashbacks, and repeated internal loops are exhausting.
A person may look into EMDR because they do not want their inner world to keep getting pulled backward by the same distressing material again and again.
8. Loss or grief still feels unfinished.
Grief is not something to “fix,” but there are times when parts of grief remain painfully unresolved or overwhelming.
EMDR may be considered when a loss still feels stuck in a way that makes it hard to remember, feel, or function without becoming flooded.
9. Talk therapy has helped, but only so much.
Many people benefit from traditional talk therapy and still want something more targeted. EMDR may feel worth exploring when a person has gained language and insight, but still feels that the deeper emotional charge has not shifted enough.
10. You want an evidence-based trauma therapy.
Some people search for EMDR specifically because they want a therapy that is recognized in major trauma treatment discussions.
EMDR is not the only strong option, but it is one of the major trauma-focused approaches people often compare when looking for treatment.
11. You want a therapy with structure.
A clear process can help some people feel safer and more focused. EMDR follows a phased approach rather than a vague or drifting session format.
That structure is one reason people find it appealing.
12. You want more freedom from triggers.
The goal is not perfection or emotional numbness. For many people, the goal is to have more choice, flexibility, and room to respond instead of being yanked around by reminders of the past.
EMDR is often considered for that reason.
13. You want the past to stop running the present.
At a deeper level, many people pursue EMDR because they want to live with more forward movement.
They want old material to feel processed enough that it no longer dominates how they think, feel, decide, or connect.
14. You want a therapy that connects memory, belief, emotion, and body.
EMDR appeals to people who do not experience distress as “just thoughts.”
It offers a framework that considers images, emotions, body sensations, and beliefs as part of the same memory network, which can feel more complete than a purely verbal approach.
15. You want help moving forward, not just understanding the past.
Many people seek EMDR because they want change that shows up in real life.
They want less reactivity, more flexibility, and a stronger sense that the past has been integrated enough for them to live differently in the present.
What EMDR is and how it works
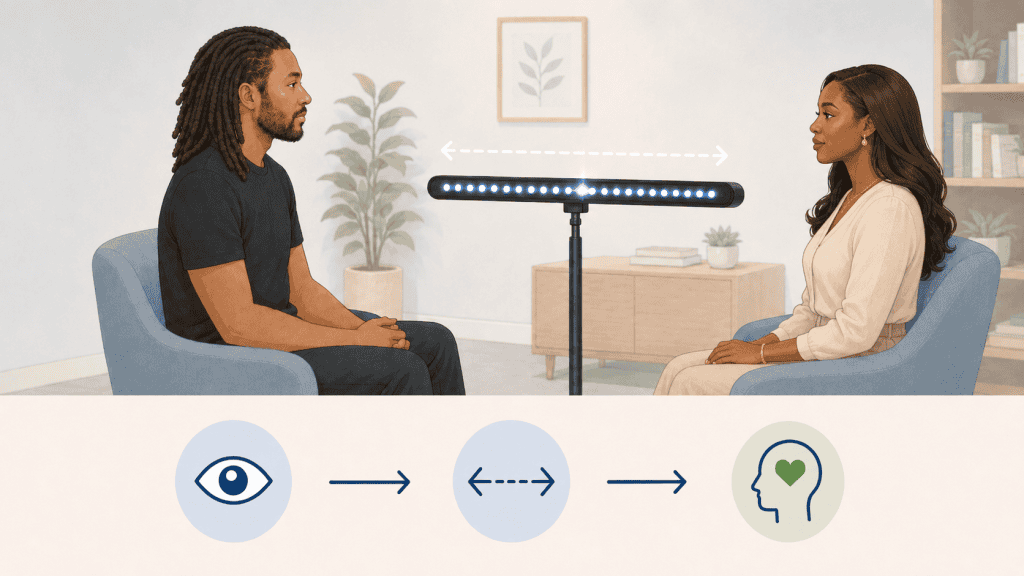
EMDR stands for Eye Movement Desensitization and Reprocessing.
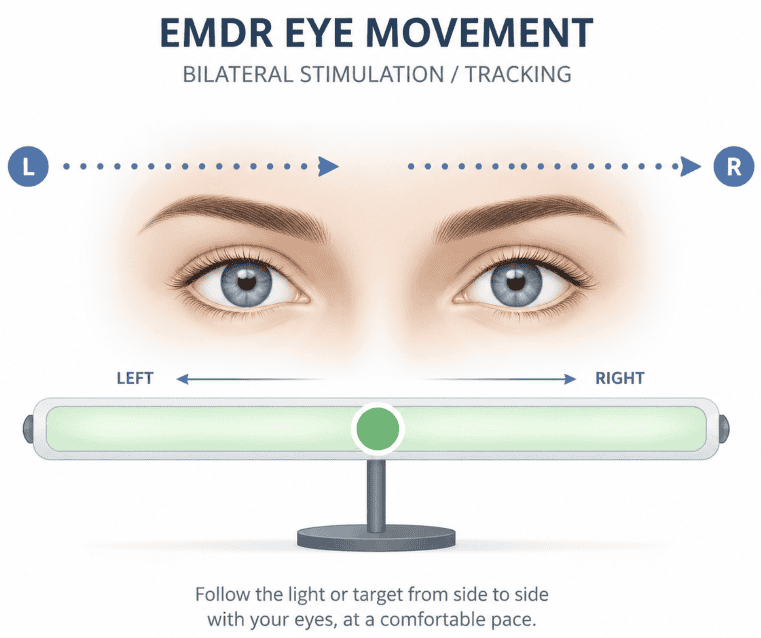
It is a structured psychotherapy that helps a person focus on a distressing memory, belief, image, emotion, or body sensation while also using bilateral stimulation such as eye movements, tapping, or tones.
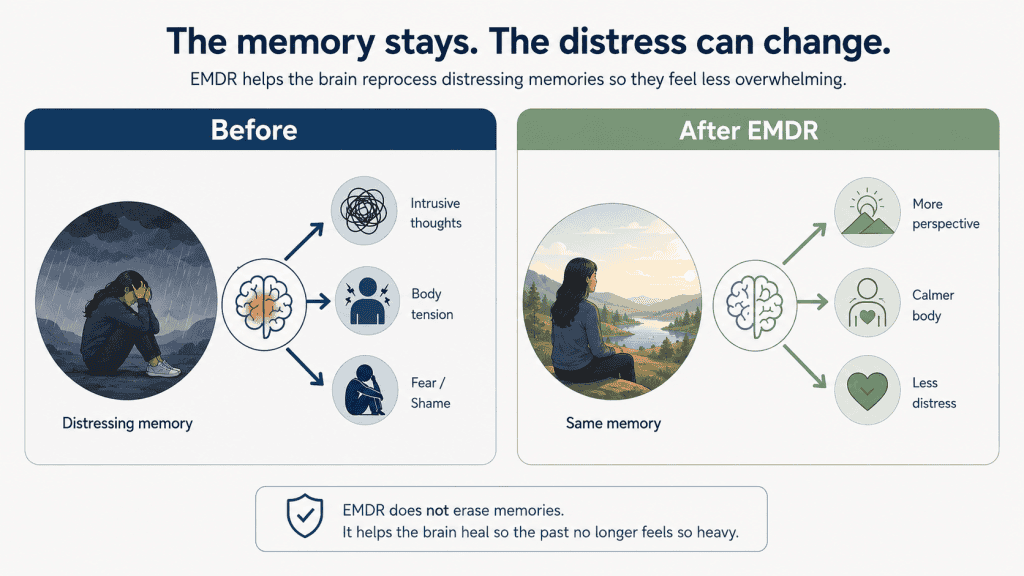
The goal is not to erase memory. The goal is to help the memory become less emotionally disruptive and more adaptively processed.
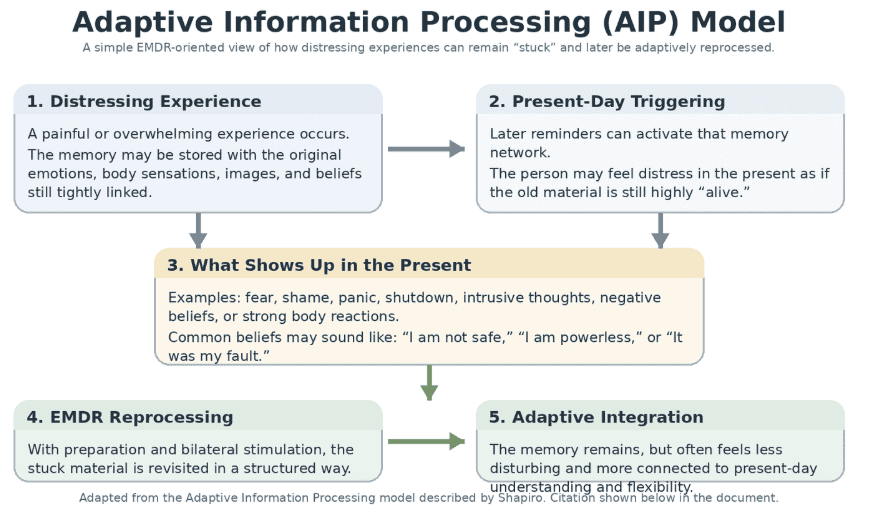
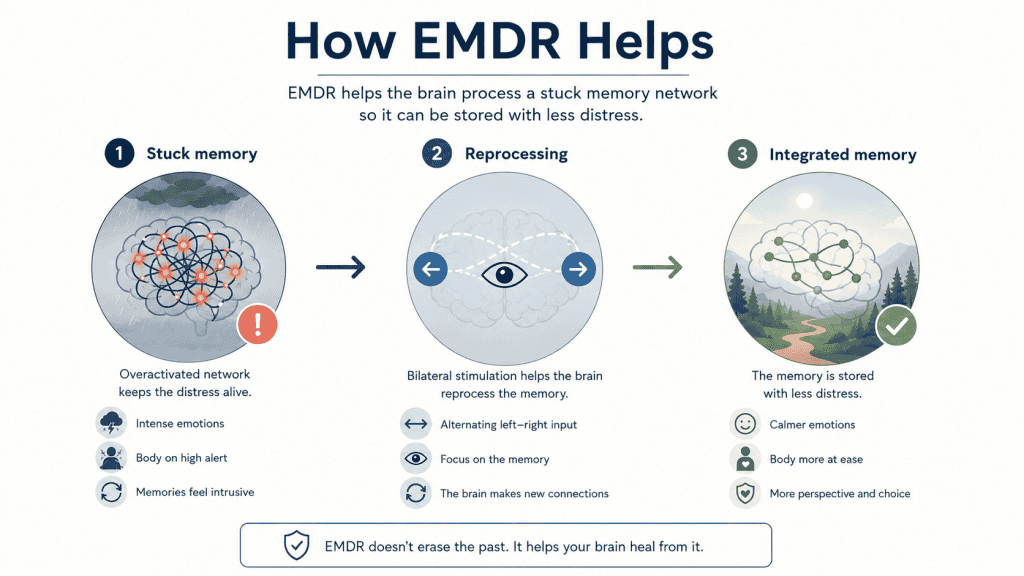
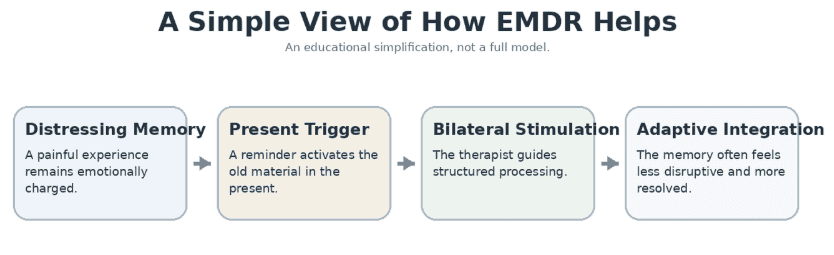
A simple way to think about EMDR is this: sometimes an experience gets “stored” in a way that keeps it emotionally raw.
A present-day trigger can then wake it up quickly. EMDR is designed to help the brain link the memory with more adaptive information so it feels less charged, less immediate, and less controlling.
What EMDR is not
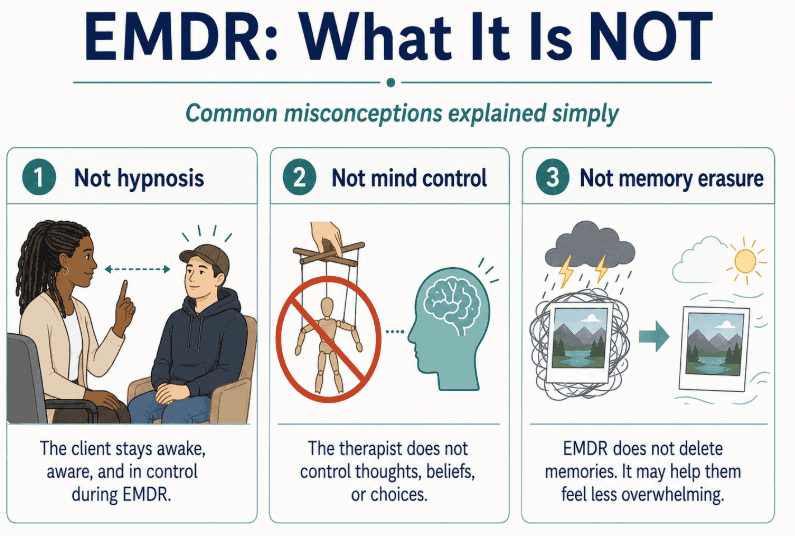
It is not hypnosis.
In EMDR, the client remains awake, alert, and in control during the session. The therapist does not put the client into a trance or direct them to surrender control.
Instead, EMDR uses a structured process where the client briefly focuses on distressing material while also paying attention to bilateral stimulation, such as eye movements, tapping, or tones.
It is not mind control.
During EMDR, the client remains aware, awake, and able to stop the process at any time. The therapist does not control the client’s thoughts, beliefs, memories, or choices.
The goal is not to control the mind, but to help the brain process painful experiences so they feel less overwhelming and less disruptive.
It is not memory erasure.
The memory does not disappear. Instead, EMDR may help reduce how painful, overwhelming, or disruptive the memory feels in the present.
It is not a magic cure or a guarantee of fast results.
It can help many people, but results vary. Some people need more time, preparation, or support. EMDR works best as a thoughtful therapy process, not as a quick fix.
It is not the right next step for every person in every phase of life.
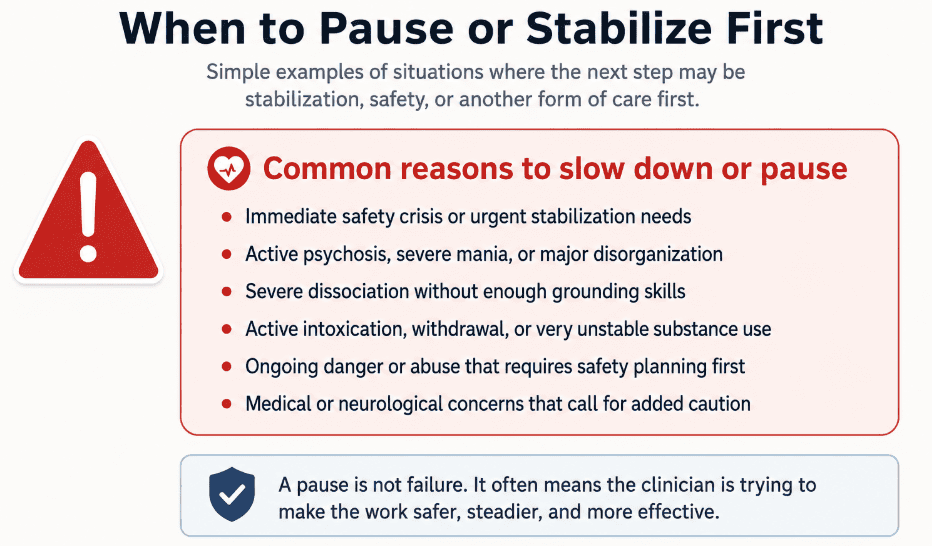
Some people may need stabilization, safety planning, grounding skills, medical support, substance-use treatment, or another form of care before beginning trauma reprocessing.
This does not mean EMDR is “bad” or that the person has failed. It means the timing, readiness, and safety of the work matter.
*EMDR is not automatically appropriate in every situation. Sometimes, the best next step is not trauma processing yet. It may be preparation, stabilization, medical support, safety planning, substance treatment, or another form of care first.
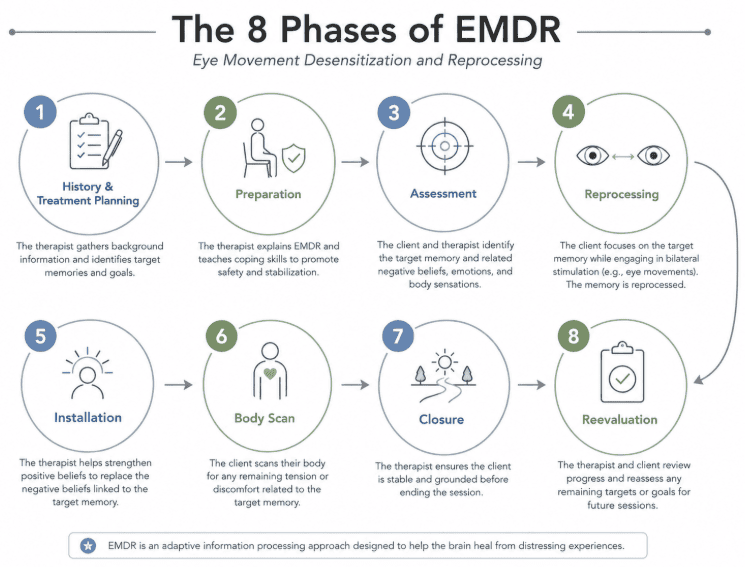
What to expect in an EMDR session
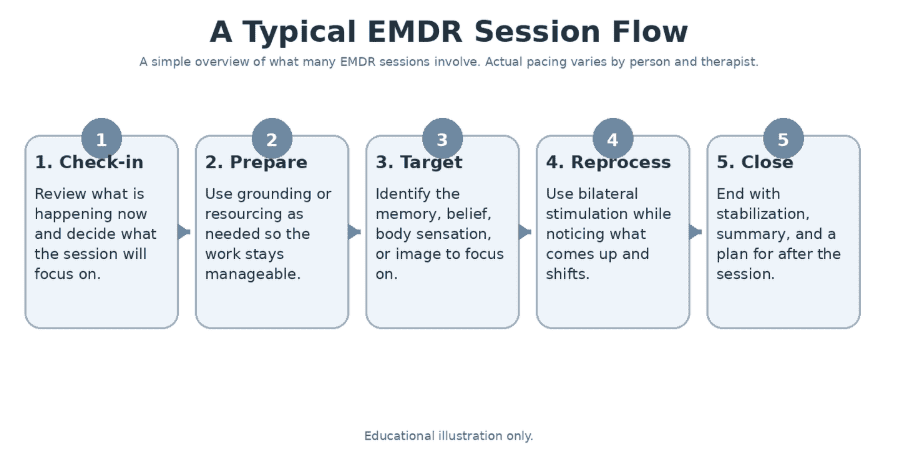
A realistic EMDR process usually involves more than jumping straight into memory processing. Many clinicians begin with history-taking, assessment, preparation, and stabilization.
That may include identifying goals, mapping target memories, learning grounding skills, and making sure the person can stay oriented if distress rises.
Once processing begins, the therapist may ask the client to bring up a target memory, a negative belief, an image, a feeling, or a body sensation while following bilateral stimulation.
The client is not expected to perform perfectly. The therapist tracks what comes up, helps the client stay anchored, and periodically checks what is shifting.
Some sessions feel relieving. Some feel tiring. Some bring up material that continues to settle after the session ends. People often need follow-up care, pacing, and stabilization – not just reprocessing.
That is why EMDR works best as a thoughtful treatment process rather than a one-size-fits-all technique.
What a good expectation sounds like
A realistic expectation is not: “This will instantly fix everything.”
A more realistic expectation is: “This may help me process stuck material in a focused way, but the pace of healing will be dependent on client’s disposition, readiness, emotional regulation ability and current living situation.”
Research Snapshot
EMDR therapy is one of the major trauma-focused psychotherapies used for PTSD. Large organizations and major treatment discussions do not treat it as fringe or experimental.
In general, research reviews and treatment guidelines tend to place EMDR alongside other leading trauma-focused therapies rather than far outside them.
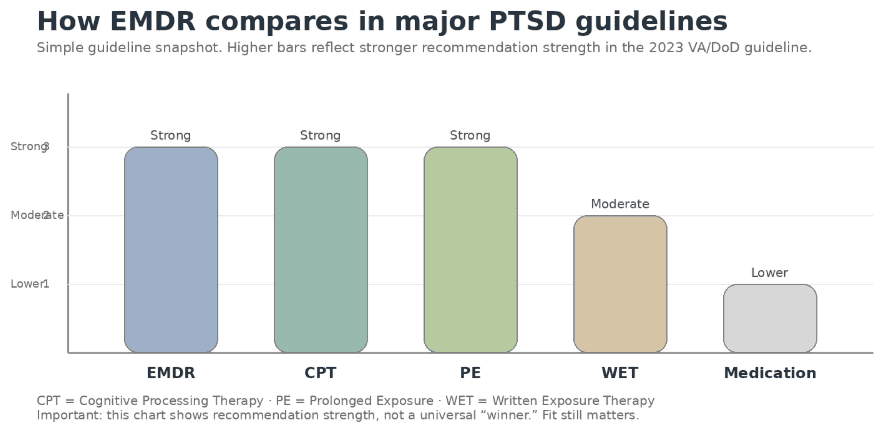
The 2023 VA/DoD PTSD guideline recommends individual trauma-focused psychotherapy over medication and specifically recommends EMDR, Cognitive Processing Therapy (CPT), or Prolonged Exposure (PE).
The World Health Organization also includes EMDR among psychological interventions to consider for adults with PTSD.
Research reviews generally find EMDR therapy effective for PTSD and roughly comparable to other leading trauma-focused approaches, while still recognizing that fit matters.
Contraindications and reasons to pause
There are many reasons to try EMDR therapy, but it is not automatically appropriate in every situation. Sometimes, the best next step is not trauma processing yet.
It may be preparation, stabilization, medical support, safety planning, substance treatment, or another form of care first.
Clinical caution note:
EMDR may need to be paused or modified when a client presents with significant instability, poor readiness for reprocessing, severe dissociation, active safety concerns, or insufficient grounding/stabilization skills. In dissociative presentations, the Francine Shapiro Legacy Library notes that certain “red flags” may contraindicate EMDR for some clients, and that safe use requires adequate preparation, informed consent, and clinical skill. Shapiro Legacy Library
EMDR FAQ
Is EMDR only for PTSD?
No. It is best known for trauma and PTSD, but it may also be used with grief, shame, anxiety, and related distress. EMDR has been found effective with a variety of mental health issues.
Is it normal to feel tired afterward?
Yes. Some people feel relieved, while others feel tired or stirred up. EMDR focuses on memory networks where past events are stored in a charged way, so feeling tired can definitely be part of the process.
Who is not a good candidate for EMDR therapy?
EMDR may not be the best first step for someone who is currently unstable, actively suicidal, severely dissociated, in active psychosis, medically unstable, or unable to stay grounded during emotional distress. In those cases, stabilization, safety planning, coping skills, and other supports may need to come first.
Do I have to talk about every detail?
Not always. Many people do not need to describe every detail for EMDR to work. Generally, only a few details are necessary. The EMDR process involves you getting inside your own head and activating existing healing capabilities.
What happens during EMDR therapy?
During EMDR therapy, you and your therapist identify a distressing memory, the negative belief connected to it, and the emotion or body sensation that comes up. While you briefly focus on that memory, the therapist uses bilateral stimulation, such as eye movements, tapping, or sounds, to help your brain reprocess the experience in a less distressing way.
Why is there a controversy with EMDR Therapy?
The controversy is not usually about whether EMDR can help trauma symptoms; it is more about why it works. Some researchers and clinicians debate whether the eye movements and bilateral stimulation are essential, or whether the benefit comes mostly from exposure, memory processing, and the structured therapy protocol.
References and useful links
For a familiar overview, see the American Psychological Association’s EMDR overview, and for context on guidelines, review the 2023 VA/DoD PTSD guideline provider summary.
American Psychological Association. (n.d.). Eye movement desensitization and reprocessing (EMDR). https://www.apa.org/ptsd-guideline/treatments/eye-movement-reprocessing
Beauvais, D., McCarthy, E., Norman, S., & Hamblen, J. L. (2023, July 18). Eye movement desensitization and reprocessing (EMDR) for PTSD. U.S. Department of Veterans Affairs, National Center for PTSD. https://www.ptsd.va.gov/professional/treat/txessentials/emdr_pro.asp
Khan, A. M., Dar, S., Ahmed, R., Bachu, R., Adnan, M., & Kotapati, V. P. (2018). Cognitive behavioral therapy versus eye movement desensitization and reprocessing in patients with post-traumatic stress disorder: Systematic review and meta-analysis of randomized clinical trials. Cureus, 10(9), e3250. https://pmc.ncbi.nlm.nih.gov/articles/PMC6217870/
Paulsen, S. L. (1995). Eye movement desensitization and reprocessing: Its cautious use in the dissociative disorders. Dissociation, 8(1), 32–44. Francine Shapiro Legacy Library.
Shapiro, F. (2018). Eye movement desensitization and reprocessing (EMDR) therapy: Basic principles, protocols, and procedures (3rd ed.). Guilford Press. https://www.guilford.com/books/Eye-Movement-Desensitization-and-Reprocessing-EMDR-Therapy/Francine-Shapiro/9781462532766
U.S. Department of Veterans Affairs & U.S. Department of Defense. (2023). VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder: Provider summary. https://www.healthquality.va.gov/guidelines/MH/ptsd/VA-DoD-CPG-PTSD-Provider-Summary.pdf
World Health Organization. (2023). Posttraumatic stress disorder (PTSD): psychological interventions – adults. https://www.who.int/teams/mental-health-and-substance-use/treatment-care/mental-health-gap-action-programme/evidence-centre/conditions-related-to-stress/posttraumatic-stress-disorder-%28ptsd%29–psychological-interventions—adults